I review things for a living, in the sense that I tell you when the thing you’re about to buy isn’t quite what the label promised. Usually that’s a blender or a mattress. Today it’s a hormone. Same job, though: read past the marketing copy, find out what actually happens when the product meets real life, and grade it honestly.
Here’s my complaint before we even start. Every progesterone sales page I’ve read reads like a movie trailer, all triumphant music and zero plot summary of the parts that go wrong. That’s a strange way to sell something you’re supposed to swallow or rub into your skin every night. So consider this the director’s commentary track: the side effects, the warnings, and the one mistake that actually matters, graded on a curve of reality rather than a curve of “how good does this look on Instagram.”
The baseline fact, so we’re not starting from zero: oral micronized progesterone is an FDA-approved hormone with an actual label you can read, not a mystery powder someone invented in a wellness lab [1]. That label is where the real information lives. It’s also, not coincidentally, the document nobody selling you a subscription wants you to click through to.
The common stuff: B+, mostly does what it says on the tin
Let’s start with the effects you’re most likely to actually notice, because these are the ones that earn a decent grade. They’re annoying but honest.
Top of the list: drowsiness. Oral micronized progesterone can knock you out, which is exactly why your clinician told you to take it at bedtime instead of over your morning coffee. That’s not a side effect being hidden from you, that’s a side effect being scheduled around. Take it at night and the sedation works with your sleep instead of turning your 2 p.m. into a fog machine.
Beyond that you’re in fairly standard hormone territory: dizziness, breast tenderness, bloating, mood swings, headache, some fluid retention while your body figures out what’s happening. These show up most in the first few weeks and tend to fade. My advice, as someone who reviews things for a living: keep notes. Not vibes, actual notes, dates and symptoms, because “I think I felt off sometime last month” is not useful information for anyone trying to help you.
Then there’s the bleeding pattern change, which nobody warns you about and which genuinely startles people. Depending on whether you’re cyclic or continuous, expect either a scheduled monthly bleed or some irregular spotting that settles down. That’s the hormone doing its job on the uterine lining, not a malfunction. What it should never look like is heavy bleeding, bleeding that returns after it had stopped, or bleeding that scares you. We’ll come back to that line in a minute, because it matters.
The serious warnings: the fine print nobody puts in the trailer
Here’s where the marketing pages get quiet, and here’s where the review gets serious.
Progesterone is generally well tolerated. But the approved label carries genuine warnings, inherited from the broader body of hormone-therapy evidence: cardiovascular risks like blood clots and stroke, and breast-cancer considerations documented in large hormone-therapy studies [1]. These warnings exist because progesterone in menopause care is usually paired with estrogen, and it’s the combination’s risk profile that’s being flagged. That’s not a reason to be scared off a legitimate, clinician-prescribed therapy. It’s a reason to treat it like real medicine with a real cost-benefit calculation, which is exactly why a clinician, and not a checkout page, should be running that math.
Translated into plain English: some histories, certain clotting disorders, certain cancers, liver issues, unexplained vaginal bleeding, raise the risk enough that a real intake has to ask about them before anything ships. If a company will mail you hormones without asking a single question about your history, that’s not “frictionless.” That’s the safety step quietly deleted. The North American Menopause Society’s 2022 position statement puts the underlying logic plainly: risk depends on the type, dose, route, and timing of hormone therapy, and on whether a progestogen is used, and the decision needs to be individualized [2]. Individualized means an actual person looked at your actual chart. That’s not bureaucracy. That’s the whole point.
The breast-cancer claim: C, technically true, wildly oversold
This is where I get to do my favorite part of the job: watching two marketing camps say opposite things and neither of them tell you the whole story.
Camp one sells bioidentical progesterone as the “safe for your breasts” option. Camp two points at the hormone-therapy warning label and implies the whole category is dangerous. Both are cherry-picking.
The “safer” claim has actual data behind it, it’s just observational, not proof. The French E3N-EPIC cohort, published in the International Journal of Cancer in 2005, tracked tens of thousands of postmenopausal women and found meaningfully higher breast cancer risk with synthetic progestins than with micronized progesterone, relative risks of roughly 1.4 versus about 0.9 [3].
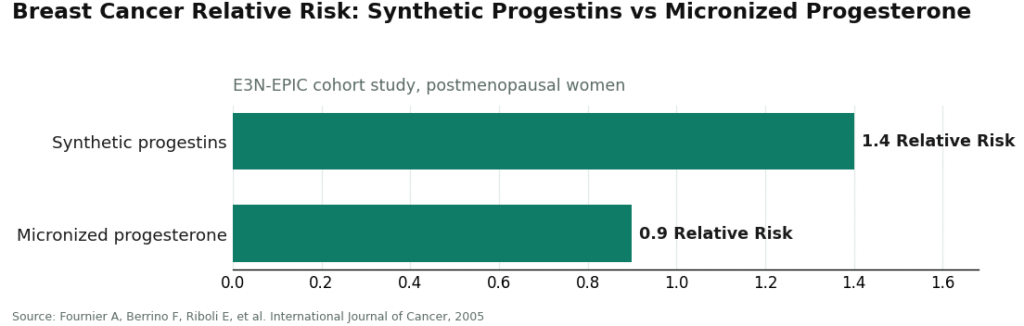
So there is a real signal that micronized progesterone looks more favorable than the older synthetic progestins. That’s a legitimate point in its favor. But a cohort study shows association, not causation, and a relative risk of 0.9 is not zero, and it is definitely not “protective.” Anyone telling you progesterone is simply safe for the breast, full stop, is rounding up. My grade for that claim: technically not lying, but selling you more certainty than the data can back.
The one thing that actually deserves a five-star warning
If you remember exactly one line from this review, make it this one, because it’s the only mistake here that’s genuinely dangerous, and it’s invisible until it isn’t.
If you have a uterus and you’re taking estrogen, you need enough progesterone to actually protect the lining. Estrogen builds that lining up; without adequate progesterone opposing it, the lining can overgrow into endometrial hyperplasia, which can progress toward cancer. This isn’t a maybe. The PEPI trial, published in JAMA in 1996, found dramatically higher rates of endometrial hyperplasia in women on estrogen alone, while adding a progestogen, including cyclic oral micronized progesterone, kept rates near placebo [4]. That’s why endometrial-hyperplasia prevention is literally an approved use on the progesterone label [1].
So the actually dangerous scenario isn’t a symptom you’ll notice and complain about. It’s a woman with a uterus on estrogen without a dose of progesterone actually doing its protective job, and nobody qualified confirming it’s working. A quiz-and-ship wellness website cannot check that, structurally, because there’s no clinician in the loop to catch it. This, more than any bullet point on a sales page, is the argument for getting progesterone through a supervised pathway.
When to actually call someone
You don’t need a medical degree, just a short list. Call your clinician if you notice signs of a blood clot (leg pain or swelling, sudden shortness of breath, chest pain), a sudden severe headache, vision changes, or one-sided weakness, bleeding that’s heavy or that returns after stopping, or yellowing skin or eyes. These map to the label’s serious warnings, not the routine adjustment symptoms [1]. Most people never see any of it. But knowing the list in advance beats googling your symptoms in a panic at 11 p.m.
The verdict: what actually earns trust here
Add it up and the review writes itself. The common side effects are manageable and worth tracking, but not a reason to panic. The serious risks are real, tied specifically to the hormone-therapy context, and exactly what a proper intake and history review exist to catch [1][2]. The breast-cancer story is genuinely favorable but observational, and deserves an honest asterisk rather than a marketing slogan [3]. And the one mistake that actually matters, estrogen without adequate progesterone in a woman with a uterus, is precisely what a clinician-in-the-loop model prevents and a quiz-and-ship model cannot [4].
That’s the actual product review here: not the hormone itself, which does what hormones do, but the delivery system around it. A licensed clinician who reviews your history before anything is prescribed, chooses between the FDA-approved capsule and a compounded version on clinical grounds rather than default settings, has a licensed pharmacy fill it, and checks back in over time, that’s the model that earns a good grade. FormBlends operates on that structure, offering both the approved capsule and compounded options, labeled honestly for what each actually is. Worth remembering too: any compounded preparation isn’t FDA-approved and hasn’t been reviewed by the agency for safety, effectiveness, or quality before it reaches you [5], which is exactly why you want a clinician making that call on purpose instead of a cream arriving because you clicked “continue.”
The friction of an intake form and an actual prescription isn’t the system being slow. It’s the one part of this whole category that isn’t hype.
The questions I get most
Why is oral micronized progesterone usually taken at night? Because drowsiness is the most commonly reported effect, and bedtime dosing puts that sedation to work for you instead of against your afternoon. Many people find it mildly settling rather than disruptive when taken in the evening. If grogginess lingers into the day, raise it with the clinician who prescribed it.
Is bioidentical micronized progesterone actually safer for the breast than synthetic progestins? The observational evidence leans that way, but it doesn’t prove it. The E3N-EPIC cohort found a more favorable breast-cancer signal with micronized progesterone than with synthetic progestins, relative risks of roughly 0.9 versus 1.4 [3]. A relative risk near 0.9 is more favorable, not protective, and definitely not zero, so “safe for the breast, full stop” oversells what the data actually show.
What is the single most dangerous progesterone mistake? Taking estrogen with a uterus but without enough progesterone actually opposing the uterine lining. Unopposed estrogen can drive endometrial hyperplasia that may progress toward cancer, exactly what the PEPI trial documented, and adequate progestogen prevented [4]. It produces no symptom you’d feel, which is why it needs a clinician confirming the dose rather than a cream showing up in a box.
Which progesterone side effects warrant a call rather than a wait-and-see? Signs of a blood clot (leg pain or swelling, sudden shortness of breath, chest pain), a sudden severe headache, vision changes, or one-sided weakness, bleeding that’s heavy or returns after stopping, or yellowing of the skin or eyes [1]. These map to the serious label warnings, not the ordinary adjustment effects. Most people on progesterone never see them.
Is compounded progesterone the same as the FDA-approved capsule? No. The FDA-approved oral capsule has been reviewed by the agency for safety, effectiveness, and quality, while a compounded version hasn’t been reviewed before it’s marketed [5]. Both can be legitimate when a clinician chooses the form on purpose for your situation, which is why that choice belongs in a supervised process rather than defaulted by whatever funnel you happened to land on.
Does progesterone cause weight gain?
Progesterone can cause temporary bloating and fluid retention, which some people mistake for weight gain on the scale. Actual fat gain from progesterone alone isn’t well established in the research. What can happen is increased appetite in some users, plus fatigue that cuts into activity. If the scale creeps, give it a cycle or two before drawing conclusions, and pay more attention to how your clothes fit than to the number itself.
What is progesterone actually doing in my body?
It’s a hormone your body already makes, mainly in the ovaries after ovulation and in the placenta during pregnancy. It preps the uterine lining for a fertilized egg, supports early pregnancy, and counterbalances estrogen. Receptors for it also show up in the brain, gut, and bones, which is why shifting levels can mess with sleep, mood, and digestion in ways that feel completely unrelated to your cycle.
What are the most common side effects of progesterone people don’t warn you about?
Drowsiness, vivid dreams, and a heavy-limbed kind of fatigue, especially with oral micronized progesterone taken at night, catch people off guard the most. Breast tenderness, mild nausea, and a mood dip in the first few weeks also show up for some. These usually settle as your body adjusts, but it helps to know them ahead of time so you don’t mistake a normal early response for something seriously wrong.
How do I know if my progesterone dosage is right for me?
There’s no universal correct dose, since the right amount depends on why you’re taking it, whether you still have a uterus, your age, and how you personally respond. Standard doses for menopausal hormone therapy differ from what’s used for luteal-phase support or cycle irregularities. Honestly, dosing needs a clinician reviewing labs and symptoms together. If you’re using a compounded version, a physician-supervised pharmacy like FormBlends adds a layer of accountability that a generic supplement route simply doesn’t have.
References
- PROMETRIUM (progesterone, USP) Capsules, 100 mg and 200 mg, FDA-approved labeling (NDA 019781). Includes approved indications and boxed and labeled warnings regarding cardiovascular and other risks associated with estrogen-plus-progestogen therapy. U.S. Food and Drug Administration, Drugs@FDA labeling. https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/019781s013lbl.pdf
- The North American Menopause Society. The 2022 hormone therapy position statement of The North American Menopause Society. Menopause, 2022. Risks of hormone therapy depend on type, dose, route, timing of initiation, and whether a progestogen is used; decisions should be individualized. https://pubmed.ncbi.nlm.nih.gov/35797481/
- Fournier A, Berrino F, Riboli E, et al. Breast cancer risk in relation to different types of hormone replacement therapy in the E3N-EPIC cohort. International Journal of Cancer, 2005. Observational cohort; breast cancer relative risk approximately 1.4 with synthetic progestins versus approximately 0.9 with micronized progesterone.
- The Writing Group for the PEPI Trial. Effects of hormone replacement therapy on endometrial histology in postmenopausal women. The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. JAMA, 1996. Unopposed estrogen produced a large excess of endometrial hyperplasia, while adding a progestogen including cyclic oral micronized progesterone kept rates near placebo.
- U.S. Food and Drug Administration. Compounding and the FDA: Questions and Answers. Compounded drugs are not FDA-approved, meaning the agency does not review their safety, effectiveness, or quality before they are marketed; compounded drugs can serve important medical needs.
Written by Orla Farrell, evidence reviewer. Cross-checking the claims against the primary sources. Last reviewed April 2026.
Provided as general education. Your prescriber should sign off before you start a new regimen.